Appendicitis is one of the most common acquired surgical conditions of childhood. Diagnosis of appendicitis remains difficult. Much work has been done on validation of clinical scores to reduce the number of unnecessary surgeries and radiographic tests while maintaining a high sensitivity for disease. However, no score performs well enough in practice to reduce these risks (Kulik et al., 2013). It is also known that appendicitis has a familial predominance, but little is known about the genetic factors that may increase a certain child's risk for the condition (Oldmeadow et al., 2009). While clearly environmental factors explain much of acquired appendicitis, the delineation of biologically factors may explain why certain patients exhibit disease, and give much more insight into the biological foundations of this illness. Unfortunately, most children presenting with appendicitis have not been referred for genetic testing unless other signs of a genetic disorder such as developmental delay or dysmorphic features are present. As a result, biologic causes of childhood appendicitis often go unrecognized, although some early work has shown that at least some biological markers exist (Muenzer et al., 2010). The addition of genetic testing results either for pre-test probability or biologic cause driven by a known genetic locus to a well standardized clinical score may make the diagnosis of appendicitis much more sensitive for the front line clinicians, therefore reducing risk for patients without the condition, and streamlining medical care for those who do.
{kind=link}
Comments
pseudocode
is a pseudocode document forthcoming for this phenotype? thanks.
portable NLP systems?
Will you be posting portable NLP systems to PheKB for these purposes:
- evaluating pathology report notes for appendicitis Case types 1 and 2
- evaluating clinical notes for reported hx of appendicitis, for case type 3 (likewise for defining controls)
many thanks!
Reported history of appendectomy
Questions:
1. For subjects that qualify as cases per NLP (case 3 per flowchart), do you want an age_at_earliest_nlp field added to the demographics table? Some of these subjects have no diagnoses or CPT codes, yet have positive NLP mention of past surgical history of appendectomy.
2. Should we exclude potential controls that do not meet case criteria, have no appendicitis diagnoses, have no control exclusion diagnoses, yet have a mention of appendectomy or appendicits via NLP?
age constraint
Are there any age constraints on this algorithm?
Thanks
Age Constraints
no, there are no age constraints. the Data Dictionary does ask for age @ diagnosis, but that's not a criteria/limitation.
Appendicitis at Harvard
We did a preliminary query and found <50 subjects with the icd9 code 540.xx
The actual number would clearly be less if we continue to apply the algorithm. So the question is whether or not to continue. Would this be too few or would it be helpful to you?
thank you for initial query.
thank you for initial query. if these samples have genome wide data, yes , we would like you to go to next step if possible.
best,
bahram
Reported History of Appendicitis
Yes, they have gtp data.
How is 'Reported History of Appendicitis' determined? I don't see codes or terms in the documentation.
Also, for the criteria 'Presence of a pathology report', 'Positive result of post-surgical biopsy report' and 'systemic antibiotics >2 days treatment', are there any timing rules associated, i.e. do the pathology report, biopsy CUIs and antibiotics need to have occurred at the same time as the appendicitis or can they have occrred any time?
Thanks
Vivian
timing question Vivian asked
Was Vivian's question ever answered? If so, can you please post it here, as we have the same question, esp. for the timing of systemic antibiotics?
thank you,
Jen
Timing , cuis and medication
If I understand your question, there isn't any timing built in to the processing of cuis. If there is a pathology report, then the cuis would come from that. We did not discriminate biopsy patholoty report vs appendectomy pathology report.
There is timing for the antibiotics. Prescription/order needs to occur on the encounter of the appendicitis diagnosis.
Reported History of Appendicitis
For Case 3, how is 'Reported History of Appendicitis' determined? Are there any specific terms or CUIS that were used?
Thanks
Initial Query at Mayo Clinic
We did the initial query using the ICD9 codes and yielded ~70 patients. Do you want us to complete the implementation?
yes, if they have genome wide
yes, if they have genome wide data, please go to the next step.
Medication typo?
I am working on the execution of the algorithm using our NLP tool suites (MedTagger and MedXN). One thing I noticed is that I could not find Mefotoxin. Is it a typo?
Perhaps. It was used in our
Perhaps. It was used in our system as an alternate name for "Mefoxin" . You should be able to find Mefoxin as RXNORM 203791.
when to check for comorbidites
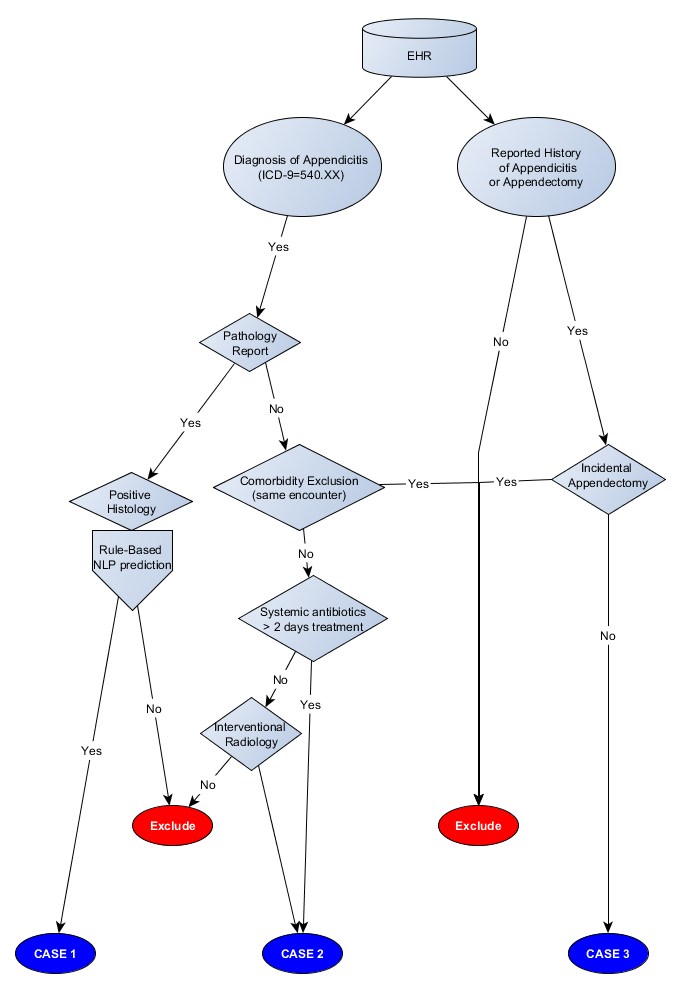
In looking closely at the flowchart diagram compared to the pseudocode for cases,
the flowchart indicates only checking for comorbdity exlcusions only if there are no pathology reports,
but the pseudocode indicates checking for this for anyone whom has a diagnosis code of 540.xx.
So, which is the correct course of action:
1) only check for comorbidities during the enc. in which diagnosed if no pathology report & exclude if they have them
OR
2) check for comorbidities for everyone w/ a diagnosis of 540.xx in that same enc. & exclude if they have them
Thank you,
Jen
Comorbidity Checking
Sorry for the confusion. The graph is correct. the psueudocode is outdated. I've updated the document here on phekb.
Only non-pathology patients get checked for comorbidities, in the Case2 branch, before medications.
Is it ok to only submit cases?
For simplicity, is it ok for us to just submit cases?
cases
We prefer a combination cases and control from each site, if possible.
keywords for history
Are there specific keywords for which we should use when searching for history of appendicitis or v?
just appendectomy & appendicitis? or also others?
I believe we just used the 1st 2 before but I want to be sure.
Thank you,
Jen
terms for CASE3
Those two terms, appendectomy and appendicitis should be sufficient. We don't have CASE 3 here in pediatric setting, so we haven't been able to validate.
Flowchart typo?
I rechecked the flowchart and now am confused. For patients with the related ICD9 codes, where should we go? Is it a typo from the node "ICD9 codes" to "Pathology Reports" (instead of no, should it be "yes")?
flowchart typo(s)?
We are assuming the pseudocode is correct, rather than the flowchart, as follows:
1) We (NU) are assuming if ICD-9 code for appendicitis = yes then check for Pathology reports .
2) Also, although it is not drawn on the flowchart, that if ICD-9 code for appendicitis = no, then, and only then look for history of appendicitis or appendectomy in encounter notes (i.e., assuming there should be an arrow labeled "no" from ICD-9 to History).
Jen
We made the same assumptions.
We made the same assumptions.
typo
Sorry for the confusion. Yes that branch from Diagnosis codes is a typo.
Case update
Todd, At the Harvard site, we have run cTAKES (NLP) to finalize our appendicitis case and control selection. We found the following numbers of cases with GWAS genotype data available among 4960 potential subjects:
Case 1: N=4
Case 2: N=2
Case 3: N= 358
Do you want us to proceed with control selection since we have so few who meet the gold standard definition (Case 1, Case 2)?
Beth Karlson
Controls Needed
Yes, controls are needed; You can focus on case3 controls, given your numbers. Thank you.
2 or 3 control types?
t see 2 control types in the algorithm, "2" & "3" -- is there a type 1?
Jen
Sorry for the confusion. In
Sorry for the confusion. In the pseudocode PDF, it's a function of the numbering. There are only 2 controls.
1. CASE
2. CONTROL
3. CONTROL(ADULT for CASE3)
cases & control types
Hi Todd,
Thank you for clarifying, that's what I thought. So I see 3 case sub-types from the flowchart, & then as you pointed out, 2 control types.
I don't like to many any assumptions if I can help it. Sharing phenotypes using narrative documents inherently leads to ambiguity, that's why we developed our phenotype authoring tool (projectphema.org) that was demonstrated with PheKB at that eMERGE webinar on 3/30. We're working on getting our NU valvular heart disease phenotype uploaded in that format, and also the phase II BPH phenotype, keep an eye out for those, and let us know what you think, and thank you for your feedback during our webinar.
Thanks, Jen
clarification on case types 1 & 2, and CPT codes?
As I said before, we were 1 of the sites in Phase II who did not run the full algorithm
(the CC simply pulled cases from the eRC whom had an ICD-9 coded diagnosis,
and controls who did not, & then we simply excluded from those controls anyone w/ keywords appendicitis or appendectomy
in their encounter notes), so this is why we have so many questions about this algorithm, as it is new to us:
For case types 1 & 2 we have 2 questions:
1) Does the appendcitis Dx have to be assoc. w/ the surgery,
OR should the pt. simply have the Dx, and have the surgery?
2) We’re using ICD-9 proc. codes to find appendectomies, but to be sure we're using the right ones,
do you have the ICD-9 procedure codes we should use (we're assuming we exclude codes for incidental appendectomies),
AND do you also have CPT codes we should use for the surgery to find case types 1 & 2?
FYI, at the moment (based on ICD-9 proc. codes, and run against our recently updated eMERGE cohort (we just added
this week 200 more subjects whom are getting WGS to our eMERGE cohort)), it looks like we have only <30 cases of type 1
at least, and don't expect many more of the other types. In addition, we only have 1 person whom can do NLP right now
(lost people & hiring new people) Thus, due to limited personnel and small case #, we are manually extracting the data
you are requesting from the pathology reports. This however should not take too long (will be faster than writing an
NLP program), we have an annotation tool to do this that just needs to be updated.
Thank you!
Jen
We didn't define the
We didn't define the appendectomy by ICD9-PROC codes, though that would be reasonable substitute for CPT codes. However, the algorithm still requires ICD-9 code diagnosis of appendicitis. That provides an initial filter for the incendental appendectomies for CASE 1s.
CPTs & Dx
ok, so did you use CPT codes to find appendectomies then, & if so, which ones?
and the ICD-9 diagnosis code & surgery don't have to be linked on same enc. &/or date?
Thanks again, Jen
ICD-9 Diagnosis + pathology
ICD-9 Diagnosis + pathology report (on same encounter-could do date too)
Case and control types
I don’t see a place in the data dictionaries to distinguish among the three case and two control types. Do you want this information? If so, can you direct me to where I can include it (if I've missed it, my apologies).
case/control files
Please provide (up to 3) separate demographics files for different case types, named case1_demo.csv, etc.
Other files can be all together. Control demographics can also be together as control_demo.csv
Please see Harvard/Partner's implementation files as an example. Thank you.